Key Counselling Points
Prior to arriving at the pharmacy for MIFE / MISO, people seeking abortion, hereinafter called "patients", will already have had a conversation with prescribers about medication abortion (MA) such as pregnancy options, eligibility, risks and efficacy[10].
When counselling patients, dispensers should provide a private space for counselling, ensure confidentiality and go over the key points below using an inclusive language[10]:
- Confirm that the decision is the patients' own, reached without coercion.
- Verify the written date of the prescription; if the prescription was written 7 or more days from when the prescription was brought to the pharmacy, the pharmacist may want to follow-up with the prescriber.
- Emphasize that in the event of an ongoing pregnancy post-MA, another dose of MISO or procedural abortion is recommended as both MIFE and MISO are teratogenic.
- Exclude contraindications.
- Review the date and time patients plan to take MIFE / MISO.
- Review the date that patients have a follow up with their prescriber.
Ensure patients have the following before leaving[10]:
- Sanitary pads and liners.
- Pain medication and/or anti-nauseants (Over-the-counter or prescription).
- Access to emergency care.
- Support for childcare, transportation, and groceries.
Ensure patients understand how to administer MIFE / MISO, how to manage side effects, and know when and how to seek care (see below).
Administration Instruction
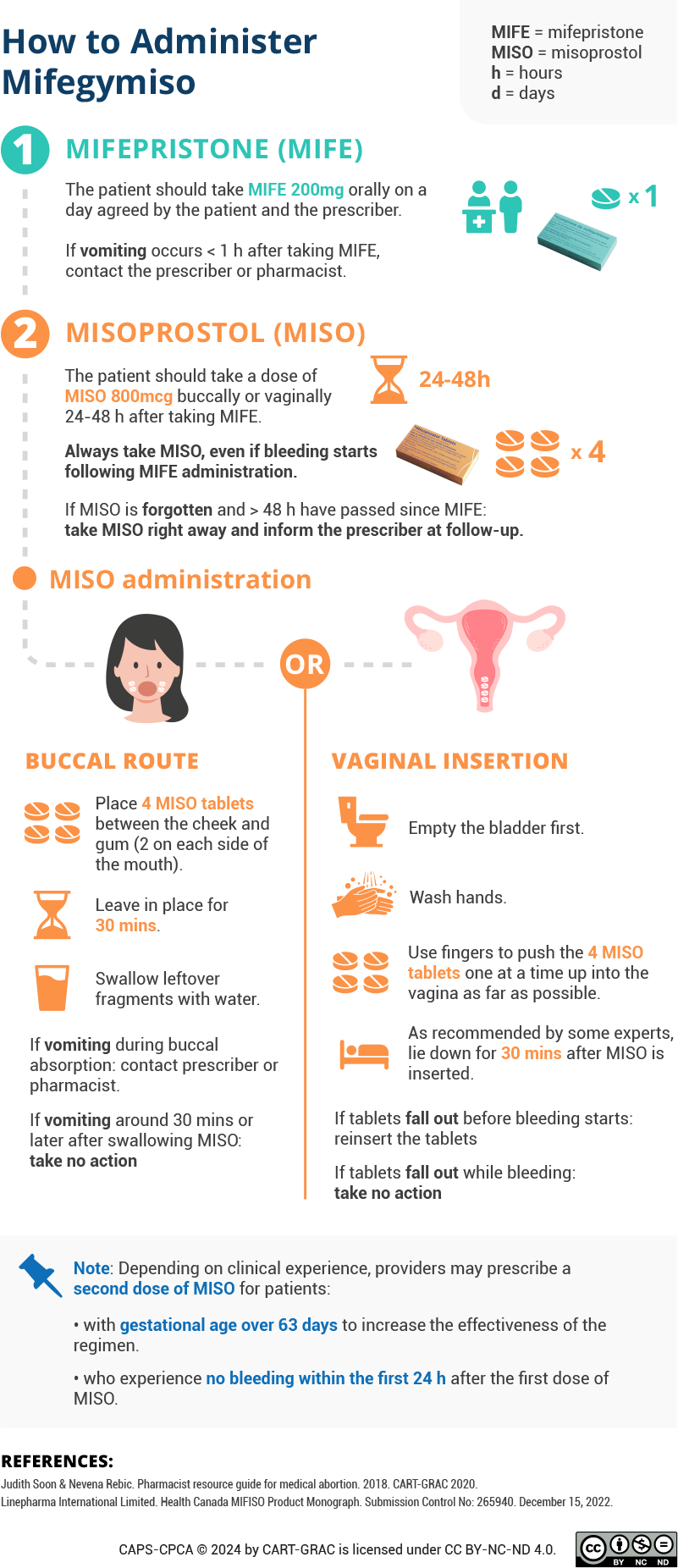
Missed Doses
Both MIFE and MISO are teratogenic and have been associated with fetal abnormalities. Once the MIFE / MISO treatment has been started, there is a risk of embryotoxicity if the pregnancy is not terminated[10].
If MISO is forgotten and > 48 hours have passed since MIFE: take MISO right away and inform the prescriber at follow-up[10].
Buccal administration of MISO[10]
- If vomiting occurs < 1 hour after taking MIFE or during buccal absorption of MISO: contact a prescriber / pharmacist for assessment.
- If vomiting occurs > 30 minutes after swallowing MISO fragments: No action is required.
Vaginal insertion of MISO[10]
- If tablets fall out before bleeding starts: Re-insert the tablet or contact a healthcare professional if unable to reinsert.
- If tablets come out while bleeding: No action is required; in most cases, a sufficient portion of the medication will have been absorbed.
In any case, if bleeding does not start within a few hours, contact a healthcare professional.
Side-effect Management

Complication Management
Ongoing pregnancy[6]: Ongoing pregnancy after medication abortion is uncommon and can be treated with another dose of MISO or with procedural abortion. Procedural abortion is recommended if cardiac activity is present 14 to 21 days after taking MISO.
Retained products of conception[6]: In the absence of ongoing pregnancy, retained products of conception can be managed by asking patients to wait for bleeding and cramping, offering them another dose of MISO, or providing them with or referring them for procedural abortion. Urgent procedural abortion is indicated in cases of heavy uncontrolled bleeding or retained products of conception associated with endometritis.
Symptoms of retained products include unexpected heavy/prolonged bleeding or cramping, and failure to have expected bleeding.
Post-abortion infections[6]: Treatment should be individualized and usually consists of broad-spectrum therapy. In mild cases, oral antibiotics can be used, but if infection is severe, patients should be hospitalized for treatment. Once patients start antibiotics, procedural abortion may be necessary to remove significant retained products of contraception.
Symptoms of Post-Abortion Infections
- Abdominal or pelvic pain
- Foul-smelling vaginal or cervical discharge
- Prolonged vaginal bleeding or spotting
- Fever or chills (more than 24 hours after MISO)
- Uterine or adnexal tenderness
- Elevated white blood cell count (upon lab examination)
Toxic shock syndrome[6]: Toxic shock syndrome is associated with clostridium and Group A streptococcus. The majority of these infections are fulminant and rapidly progress to shock. Standard antibiotic therapy is not sufficient; thus, the treatment consists of supportive care, and empiric antibiotic treatment covering clostridial species and other organisms known to cause toxic shock, and surgical debridement, including possible hysterectomy.
Symptoms of Toxic Shock Syndrome
- General malaise with nausea, vomiting, and diarrhea
- Absence of fever (or mild fever)
- Minimal abdominal pain
- Weakness
- Flu-like symptoms
- Tachycardia / hypotension
- Edema
- High white blood cell counts or high hemoglobin level (upon lab examination)
Optional Follow-Up
Patients are required to have a follow-up consultation with prescribers.
A follow-up with dispensers is optional and can take place 2 – 3 days after MISO administration. During the follow-up, dispensers can do the following[9,10]:
- Verify appropriate administration
- Review side effect management
- Review contraception options
- Reinforce prescriber follow-up
- Provide emotional support
Emotional response after MA often vary. Some people feel relieved and positive and some have feelings of grief, sadness, or guilt while others have mixed feelings. These emotions are normal, and they may or may not be related to socioeconomic circumstances, the lack of social support, moral discomfort, and family conflict.
Patients can be supported by understanding that mixed emotions are normal and by exploring coping strategies and support. Useful resources include:
- Exhale, a talk-line that provides emotional support, resources and information after abortion.
- All-Options, a talk-line to discuss past or current experience with abortion, adoption and parenting for people in Canada and the United States (1-888-493-0092).
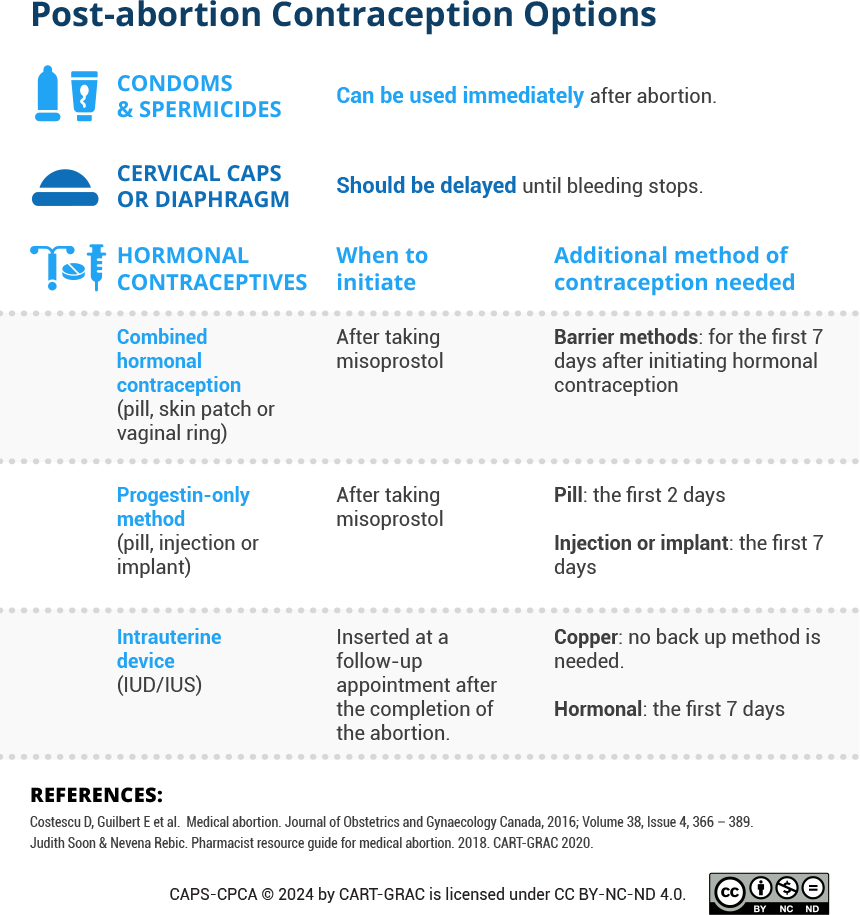
Post-abortion Contraception
Due to rapid return to fertility following medication abortion (MA), patients should be advised to have a method for contraception at the earlier visits[6].
Patients seeking more information about contraception options can be referred to:
- Sex and U’s It’s a plan, an online health information tool to determine the right contraception method.
- Action Canada’s Sexual Health Hub on Birth Control, a website that contains information on birth control in Canada.
Below is a list of contraception options and special considerations: